

developmental cysts mean that they are of uncertain origin on the reverse of inflammatory cysts that are associated with inflammation as in radicular cyst in which bacteria from pulp stimulate inflammatory response ,hence inflammatory cells release cytokines as messengers to fibroblasts in cyst wall that release prostaglandins & collagenese so cyst expansion by bone resorption and all this with the aid of Osmosis as we mentioned before, another scenario as in the paradental cyst which is also inflammatory cyst associated with pericoronitis.
1-Dentigerous cyst(Follicular cyst).
 -Dentigerous cyst is the most common developmental cyst and the second most common odontogenic cyst after radicular cyst.
-Dentigerous cyst is the most common developmental cyst and the second most common odontogenic cyst after radicular cyst. BUT, although all dentigerous cysts are to be developmental in origin ,there are some examples that appear to have an inflammatory pathogenesis i.e dentigerous cyst may develops around unerupted permanent tooth as a result of periapical inflammation from an overlying primary tooth. Another similar scenario involved paradental cyst or buccal bifurcation cyst.
BUT, although all dentigerous cysts are to be developmental in origin ,there are some examples that appear to have an inflammatory pathogenesis i.e dentigerous cyst may develops around unerupted permanent tooth as a result of periapical inflammation from an overlying primary tooth. Another similar scenario involved paradental cyst or buccal bifurcation cyst. 1)Dentigerous cyst is adevelopmental cyst but there are some cases that are inflammatory i.e periapical inflammation of decidous tooth may stimulate cystic changes of the underlying permanent one causing inflammatory dentigerous cyst
1)Dentigerous cyst is adevelopmental cyst but there are some cases that are inflammatory i.e periapical inflammation of decidous tooth may stimulate cystic changes of the underlying permanent one causing inflammatory dentigerous cyst -Dentigerous cyst may occur around ay unerupted tooth but most often it involves mandibular 3rd molar ,other frequent site include maxillary canine , maxillary 3rd molar ,mandibular premolars respectively.
Radiographic picture,
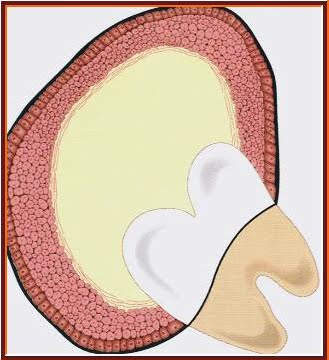
-Dentigerous cyst appears as well-defined unilocular radiolucent area associated with crown of unerupted tooth. A large dentigerous cyst may give the impression of multilocular appearance because of the persistence of bone trabeculea within the radiolucency ( pseudoloculation of bone trabeculea) however ,dentigerous cyst are grossly and histologicaly unilocular and never are truly multilocular.
associated with crown of unerupted tooth. A large dentigerous cyst may give the impression of multilocular appearance because of the persistence of bone trabeculea within the radiolucency ( pseudoloculation of bone trabeculea) however ,dentigerous cyst are grossly and histologicaly unilocular and never are truly multilocular.
-The affected unerupted tooth usually displaced,it may also  displace or resorp root of adjacent erupted tooth.
displace or resorp root of adjacent erupted tooth.
-The cyst to crown relationship shows several radiographic variations :
a) central type : the most common type, the cyst is completely surround the crown
b) lateral type : the cyst projects laterally from the side of the tooth.
c)circumferential type: the cyst durround the crown and extends around the roots so portion of roots appear to lie within the cyst.


-Radigraphic picture is not diagnostic for dentigerous cyst, keratocyst,unilocular ameloblastome and other odontogenic & nonodontogenic tumors have radiographic pictures identical to those of a dentigerous cyst.

Dentigerous cyst associated with premolar
Cyst expansion,
Mechanism of expansion si,ilar to that of radicular cyst by osmosis and bone resorption
 Histopathology,
Histopathology,
histopathology varies depending on whether the cyst is inflammatory or developmental, in the common non inflammed dentigerous cyst, the lining is thin , regular ,nonkeratinized stratified squamous epithelium, may flattened or low cuboidal,mucous cells may be found in epithelial lining as a result of mucous metaplasia of epithelial cells, the connective tissue capsule of the cyst free from inflammatory cells and there are islands of odontogenic epithelial rests may be seen.


Islands of odontogenic epith. within cyst wall

Lining of ciliated stratified may be seen

Mucous cells within lining due to metaplasia

Inflammatory dentigeous cyst
Treatment,
the usual treatment is enucleation with removal of unerupted tooth, the cyst may be treated by marsupialization when the tooth is allowed to erupt or if it can be orthodontically guided to its position in the arch.and in case of large dentigerous cyst.
Prognosis,
prognosis of dentigerous cyst is excellent and recurrence is seldom occurs. However ,several complication may be noted, dentigerous cyst may complicate to:
1)Ameloblastoma (lining of the cyst may undergoes neoplastic transformation)
2)Squamous cell carcinoma (due to mucous metaplasia)
3)Intraosseous mucoepidermoid carcinoma (due to mucous metaplasia)
..................................................................................































{kind=link}